Understanding the Surgical Mechanism
One of the key factors contributing to erectile dysfunction (ED) is venous leakage in the penile veins. During normal erection, arterial vessels dilate, and smooth muscles within the corpus cavernosum relax, allowing a large volume of blood to fill the penis, resulting in rigidity.
However, if the penile venous system fails to close, blood leaks out of the erectile tissue too quickly, leading to weak erections, insufficient hardness, or rapid detumescence. The severity of the venous leak directly affects the rigidity of the erection.
The goal of penile venous ligation surgery is to block the outflow of venous blood, thereby increasing blood retention in the corpus cavernosum and enhancing erection firmness during sexual activity.
Anesthesia Technique
The procedure uses dual local anesthesia, including dorsal penile nerve block and peri-penile base tissue block, performed only at the penile base (Figure 1).
Patients remain awake and pain-free throughout the operation—using a phone or Bluetooth headset is allowed during surgery.
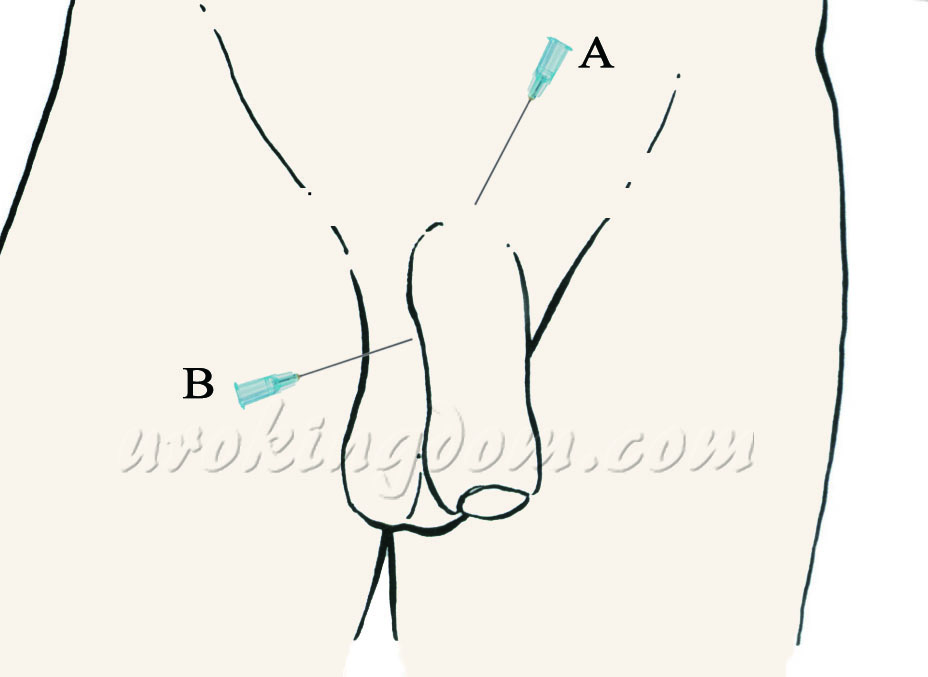
Figure 1: Dual local anesthesia – dorsal penile nerve block (A) and peri-penile base block (B), performed only at the base of the penis.
Surgical Incision
A single 3 cm incision is made at the suprapubic area (just above the pubic bone).
If circumcision is performed simultaneously, a secondary incision is made below the glans (coronal sulcus).
Hospital Stay
No hospitalization is required.
Patients can walk and return home shortly after the surgery.
Surgical Technique and Procedure
Performed in the supine position under precise local anesthesia, the surgery is guided by the latest anatomical insights into the penile venous system (Figure 2).
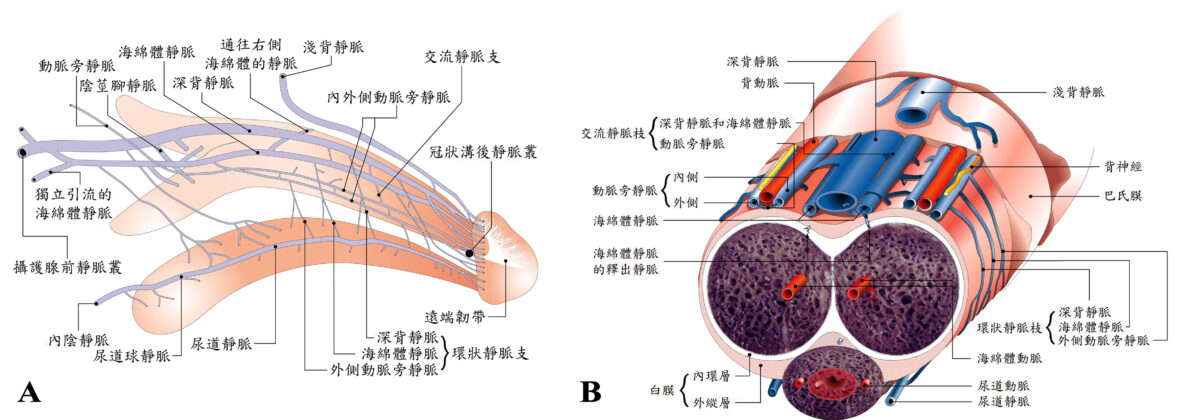
Using microsurgical techniques, a 3 cm vertical incision is made at the midline of the suprapubic skin. If combined with circumcision, a separate foreskin incision is added.
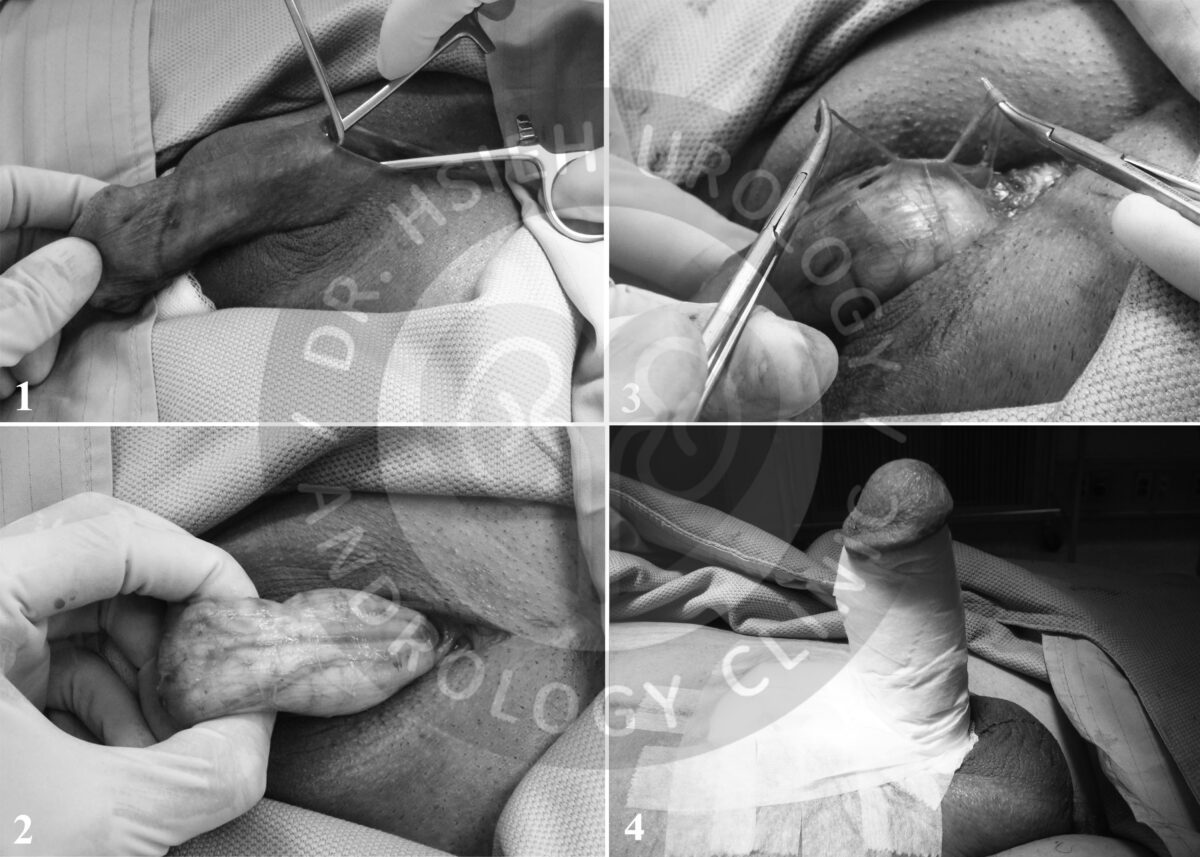
The penile shaft is carefully exposed and everted. With microsutures, the deep dorsal vein and cavernosal veins are ligated and removed.
Smaller veins (e.g., para-arterial, circumflex, and crural veins) are also tied off to fully block venous outflow.
The penile shaft is repositioned, and the incision is closed with fine sutures, then wrapped in sterile gauze (Figure 3).
During the operation, the superficial dorsal vein and bulbourethral veins are preserved to maintain healthy penile blood circulation.
Hemostasis is achieved using microsutures—no electrocautery is used, reducing the risk of thermal injury to adjacent arteries and nerves.
Our Surgical Advantages
- Dual local anesthesia
- Single minimal incision
- No hospitalization required
- Guided by the most accurate penile venous anatomical data
- No electrocautery—minimizing tissue damage and complications
- Microsurgical precision for optimal safety and healing
Postoperative Outcomes
Earlier reports of traditional penile venous surgeries showed short-term improvement rates of 50–80%.
However, long-term success rates dropped to 31–64% due to factors like incomplete vein ligation, smooth muscle dysfunction, or aging.
With enhanced penile venous ligation and careful patient selection, long-term results have been encouraging:
- 90.4% reported improvement in erectile function
- 87.9% satisfaction rate
- Statistically significant improvement in IIEF (International Index of Erectile Function) scores
Only mild and temporary complications were observed, such as lymphatic swelling, bruising, or transient palpitations related to local anesthesia.
No major complications were reported in long-term follow-up.
Conclusion: A Reliable Option for Venous Leak in Erectile Dysfunction
Venous leakage is a major cause of erectile dysfunction. With in-depth understanding of penile venous anatomy, enhanced penile venous ligation surgery provides more complete and lasting results compared to traditional methods.
This procedure remains a viable and valuable option for patients carefully selected based on favorable surgical conditions. Many can achieve spontaneous, natural erections without the need for medication or devices.
Integrating penile venous surgery into a comprehensive treatment strategy—including counseling, oral PDE5 inhibitors, low-intensity shockwave therapy, and hormone replacement—maximizes outcomes for ED patients.
If all other methods fail, penile prosthesis implantation remains a final yet effective solution.
期刊論文
- Hsu GL(許耕榕), Hsieh CH(謝政興), Chen HS, Ling PY, Wen HS, Liu LJ, Chen CW, Chua C. The advancement of pure local anesthesia for penile surgeries: can an outpatient basis be sustainable (純粹局部麻醉施行陰莖手術的新進展). Journal of Andrology. 28(1):200-205, 2007.
- Hsu GL, Zaid UX, Hsieh CH (謝政興), Huang SJ. Acupuncture assisted local anesthesia for penile surgeries (針灸輔助局部麻醉下施行陰莖手術). Translational Andrology and Urology. 2(4):291-300, 2013.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Hsu WL, Chen YC, Chen RM, Chen SC, Hsieh JT. The effect of electrocoagulation on the sinusoids in the human penis (電燒止血對於人類陰莖海綿體的影響). Journal of Andrology. 25(6):954-959, 2004.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Chiang HS. Penile venous anatomy: application to surgery for erectile disturbance (陰莖靜脈解剖構造:在勃起功能障礙手術中的應用). Asian Journal of Andrology. 4(1):61-66, 2002.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Chen YC, Chen SC, Mok MS. Penile venous anatomy: an additional description and its clinical implication (陰莖靜脈解剖構造:附加描述及其臨床意涵). J Androl. 2003; 24: 921-927.
- Hsu GL(許耕榕), Hsieh CH(謝政興), Wen HS, Hsu WL, Wu CH, Fong TH, Chen SC, Tseng GF. Anatomy of the human penis: the relationship of the architecture between skeletal and smooth muscles (人類陰莖解剖構造:骨骼肌和平滑肌之間的結構關係). Journal of Andrology. 25:426-431, 2004.
- Hsieh CH(謝政興), Wang CJ, Hsu GL(許耕榕), Chen SC, Ling PY, Wang T, Fong TH, Tseng GF. Penile veins play a pivotal role in erection: the hemodynamic evidence (陰莖靜脈在勃起中扮演關鍵角色:血液動力學上的證據). International Journal of Andrology. 28(2):88-92, 2005.
- Chen SC, Hsieh CH(謝政興), Hsu GL(許耕榕), Wang CJ, Wen HS, Ling PY, Huang HM, Tseng GF. The progression of the penile vein: could it be recurrent (陰莖靜脈的進展:陰莖靜脈手術後是否會復發)? Journal of Andrology. 26(1):53-60, 2005.
- Wen HS, Hsieh CH(謝政興), Hsu GL(許耕榕), Kao YC, Ling PY, Huang HM, Wang CJ, Einhorn EF. The synergism of penile venous surgery and oral sildenafil in treating patients with erectile dysfunction (陰莖靜脈截除手術與口服威而剛治療勃起功能障礙的協同作用). International Journal of Andrology. 28(5):297-303, 2005.
- Hsu GL(許耕榕), Chen HS, Hsieh CH(謝政興), Lin PL, Wen HS, Liu LJ, Chen CW, Liu MW. Insufficient response to venous stripping surgery: is the penile vein recurrent or residual (陰莖靜脈截除手術後反應不佳:陰莖靜脈復發或殘留?). Journal of Andrology. 27(5):700-706, 2006.
- Hsu GL(許耕榕), Chen HS, Hsieh CH(謝政興), Lee WY, Chen KL and Chang CH. Salvaging penile venous stripping surgery (陰莖靜脈截除挽救手術). Journal of Andrology. 31(3):250-260, 2010.
- Hsu GL(許耕榕), Chen HS, Hsieh CH(謝政興), Lee WY, Chen KL and Chang CH. Clinical experience of a refined penile venous stripping surgery procedure for patients with erectile dysfunction: is it a viable option (精煉的改良式陰莖靜脈截除手術治療勃起功能障礙的臨床經驗:手術是可行的選擇?). Journal of Andrology. 31(3):271-280, 2010.
- Hsu GL(許耕榕), Hung YP, Tsai MH, Hsieh CH(謝政興), Chen HS, Molodysky E, Huynh CC, Yu HJ. Penile veins are the principal component in erectile rigidity: a study of penile venous stripping on defrosted human cadaver (陰莖靜脈是達成勃起硬度的主要因素:在解凍的人類屍體上進行陰莖靜脈截除手術的研究). Journal of Andrology. 33:1176-1185, 2012.
- Hsieh CH(謝政興), Hsieh JT, Chang SJ, Chiang IN, Yang SSD. Penile venous surgery for treating erectile dysfunction: past, present, and future perspectives with regard to new insights in venous anatomy (陰莖靜脈手術治療勃起功能障礙的過去、現在與未來:陰莖靜脈解剖學的新見解). Urological Science. 27(2):60-65, 2016.
- Hsieh CH(謝政興), Hsu GL(許耕榕), Chang SJ, Yang SSD, Liu SP, Hsieh JT. Surgical niche for the treatment of erectile dysfunction (手術治療勃起功能障礙的利基). International Journal of Urology. 2020; 27: 117-133.
書籍著作
- Cheng-Hsing Hsieh (謝政興), Geng-Long Hsu. Current role of vascular surgery (arterial and venous) in erectile dysfunction (當前動脈及靜脈血管手術在勃起功能障礙中的角色), in INTERNATIONAL BOOK OF ERECTILE DYSFUNCTION, M.L. Djordjevic and F.E. Martins, Editors. 2016, Nova Science Publishers, Inc.: New York. chap. 9, pp. 129-157. ISBN: 978-1-63485-289-0
- Geng-Long Hsu, Cheng-Hsing Hsieh (謝政興), Eric Allaire. Vascular (Arterial and Venous) Surgery for Erectile Dysfunction (血管(動脈與靜脈)手術治療勃起功能障礙), in Textbook of Male Genitourethral Reconstruction, Francisco E. Martins, Sanjay B. Kulkarni and Tobias S. Köhler, Editors. 2020, Springer Nature: Switzerland AG. chap. 50, pp. 663-678. ISBN: 978-3030214463
- Cheng-Hsing Hsieh (謝政興)、Geng-Long Hsu (許耕榕). 治療勃起功能障礙 – 手術治療(Erectile Dysfunction – Surgical Management).書名:男性性功能障礙 – 臨床診治全攻略 (Male Sexual Dysfunction – A Complete Guide to Diagnosis and Treatment), 陳煜、簡邦平、蔡維恭、陳卷書編輯. 合記圖書出版社, 2023. 第三篇,第17章,頁245-262.
- Cheng-Hsing Hsieh (謝政興)、Geng-Long Hsu (許耕榕). 勃起功能障礙 – 手術治療 (Erectile Dysfunction – Surgical Treatment). 書名:臨床泌尿學 (CLINICAL UROLOGY).郭漢崇、賴明坤、楊啟瑞、黃一勝、余燦榮、陳進典、崔克宏,編輯. 台灣泌尿科醫學會, 2012.第八篇,第54章,頁1037-1049.
- Geng-Long Hsu (許耕榕)、Cheng-Hsing Hsieh (謝政興). 書名:A LABORATORY MANUAL FOR POTENCY MICROSURGERY (性功能顯微手術實驗訓練手冊). 許耕榕、謝政興,編輯.
參考文獻
- Das S. Early history of venogenic impotence. Int J Impot Res. 1994; 6: 183–189.
- Wespes E, Schulman CC. Venous leakage: surgical treatment of a curable cause of impotence. J Urol. 1985; 133: 796-798.
- Lue TF. Penile venous surgery. Urol Clin North Am. 1989; 16: 607-611.
- Lue TF. Surgery for crural venous leakage. Urology. 1999; 54: 739-741.
- Bennett AH, Rivard DJ, Blanc RP, Moran M. Reconstructive surgery for vasculogenic impotence. J Urol. 1986; 136: 599-601.
- Berardinucci D, Morales A, Heaton JP, Bloom S. Surgical treatment of penile veno-occlusive dysfunction: is it justified? Urology. 1996; 47: 88-92.
- Montague DK, Barada JH, Belker AM, et al. Clinical guidelines panel on erectile dysfunction: summary report on the treatment of organic erectile dysfunction. The American Urological Association. J Urol. 1996; 156: 2007-2011.
- Hsu GL, Hsieh CH, Wen HS, Chen YC, Chen SC, Mok MS. Penile venous anatomy: an additional description and its clinical implication. J Androl. 2003; 24: 921–927.
- Hsu GL, Hung YP, Tsai MH, et al. Penile veins are the principal component in erectile rigidity: a study of penile venous stripping on defrosted human cadavers. J Androl. 2012; 33: 1176-1185.
- Hsu GL, Chen HS, Hsieh CH, Lee WY, Chen KL, Chang CH. Clinical experience of a refined penile venous stripping surgery procedure for patients with erectile dysfunction: is it a viable option? J Androl. 2010; 31: 271-280.
- Hsieh CH, Hsu GL, Chang SJ, Yang SSD, Liu SP, Hsieh JT. Surgical niche for the treatment of erectile dysfunction. Int J Urol. 2020; 27: 117-133.
- Hwang TI, Yang CR. Penile vein ligation for venogenic impotence. Eur Urol. 1994; 26: 46.
- Hsu GL, Chen HS, Hsieh CH, et al. Insufficient response to venous stripping surgery: is the penile vein recurrent or residual? J Androl. 2006; 27: 700-706.